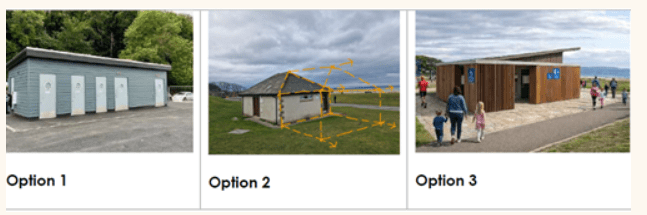
There will be several Stakeholder meetings and future Public Consultation meetings. NICE will be looking at the proposed draft plans and the future sustainability of the toilet building. The final decision to go ahead with the project, although many months away, will consider things like ownership, financing, security as well as ensuring adequate support from organisations like the Council, Government bodies and local businesses to ensure its continuous viability.
A stakeholder workshop regarding the proposed redevelopment of the public toilet facilities at Nairn Link has been arranged for Wednesday 18 March 2026. Nairn Improvements Community Enterprise (NICE) Nairns Enterprise Company have engaged Colin Armstrong Architects to draw up plans for the new toilet facility. Nairn River Community Council (NRCC) will be attending as stakeholders on the project. Follow this link to see the first draft of the design brief. Please email info.nrivercc@gmail.comwith any comments or suggestions and they will be passed on to the NICE team and to the architects.
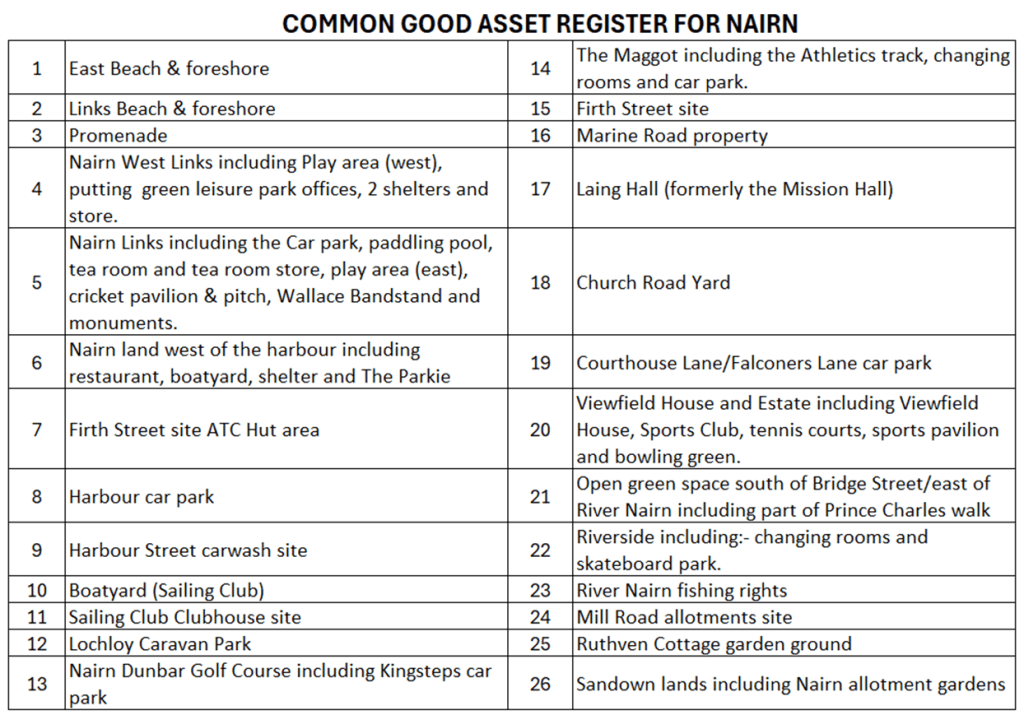
Nairn Common Good Fund set up for benefit of former Burgh of Nairn.
Financial information about this fund is contained within the Annual Accounts and Area Committee monitoring reports which are available on the Highland Council website.
Monuments and Other Assets
Market Cross
The Toorie
Poet’s Well
3rd Division Infantry Stone
Dr Grigor statue
Provost Chains of Office
Portrait – Viscount Finlay
Painting of Nairn from the River (from Jubilee Bridge)
Painting of D Sub Section Inverness Battery RHA Palestine (1914-1918)
Monday 5 January had a crystal clear blue sky, the day was cold and bright as the sun was shining, there is no doubt as to what was washed ashore. What is shown in the photographs below is brown, foul smelling sewage mulch. It was at least 5/6 inches deep in places and occurred over most of the Nairn East beach right up to access point 9 and beyond. NRCC wrote to SEPA and Public Health Highland to register our concerns.
Nairn River Community Council (NRCC) has major concerns about sewage discharges and public health concerns at Nairn East beach.
Nairn has once again experienced the troubling issue of raw sewage being washed ashore onto its beach. This recurring problem has caused concern among local residents and visitors, drawing attention to the ongoing challenges with sewage management in the area.
The affected location is situated in the vicinity of the sewage pipe that runs from the Nairn Wastewater Treatment Works to the designated discharge point. It is evident that raw sewage has likely washed ashore, a direct consequence of the sewerage pipe being broken in multiple places.
This situation is not only disgraceful but represents an extremely serious public health concern. Scottish Water holds the responsibility for ensuring that such incidents do not occur; however, these events have been repeated on several occasions. The links provided below illustrate that problems with this outfall pipe have persisted for a considerable period.
There is a clear necessity for Public Health Highland and SEPA to conduct investigations into this significant spill. Repair work on the outfall commenced on Monday, 19 May 2025, but further damage was discovered in subsequent months across other sections of the outfall pipe. Consequently, the repair efforts have been halted, with no indication as to when they will resume or be completed.
Given its responsibility for addressing potential environmental hazards to health, Public Health Highland must investigate this major spill as a matter of urgency.
NRCC asserts that Scottish Water has breached its license (NGR NH 8930 5830) by delaying and failing to complete the necessary repairs properly. NRCC also believes SEPA should conduct an independent investigation into these shortcomings by Scottish Water.
NRCC understands that both Public Health Highland and SEPA work closely with Scottish Water.
It would be helpful if you could share this link through your social media channels and with any local groups or organisations within the community to help our customers and your constituents understand what is happening.
Customer information materials will also be available in branch.
This email is being sent as a service message. If you have previously opted out of receiving marketing communications from Post Office that opt out remains in place.
Post Office Limited is registered in England and Wales number: 2154540 Registered Office: 100 Wood Street, London, EC2V 7ER
At the Highland Council meeting on 15 May 2025 the “Review of the Highland Scheme of Establishment for Community Councils 2024/25 – Phase 1 Feedback” appeared on the agenda.
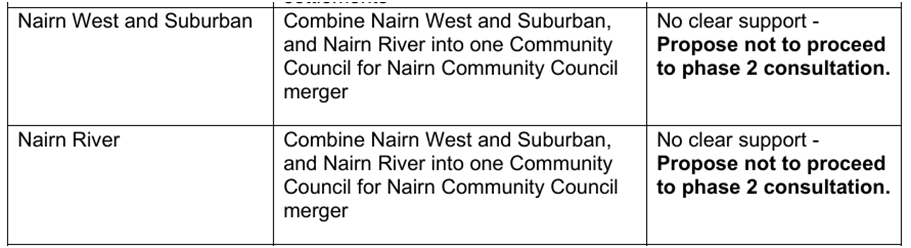
The most important item on the scheme for NRCC was the proposed forced merger of ‘NRCC’ and ‘Nairn West and Suburban CC’ to make one CC for the 10 000 plus residents of Nairn. The proposed CC would have been the biggest in the Highlands by far.
Neither NRCC nor NW&SCC were advised of this attempted nefarious act before THC had their ‘Special Meeting’ in December 2024 where the Council were presented with the Scheme Review. Many of our sister CCs, throughout the Highlands, submitted a comment that they were against this merger as being undemocratic and immoral.
NRCC and NW&SCC work closely together when any issues raised would have an effect on Nairn Town-wide, Tourism, Common Good matters and so forth but neither group were agreeable to the merger. CCs have no Authority over the Council nor over the local members but continuously suffer from those looking for someone to blame for the shortfalls Nairn suffers at the hands of the Highland Councils lack of funding for Nairn compared to smaller towns around the Highlands.
THC have “proposed not to proceed to phase 2 consultation” as there was “No clear support” or to put it another and probably a more correct way, they received many more comments against the proposal than were for the proposal.
Perhaps it is time for those who advocated a single CC for Nairn, including our own Provost, should now put their time and efforts, (especially that spent on facebook) in campaigning for the breakup of Highland Council. Nairn would have its own Council and be answerable to the People and not be governed by faceless officials in Inverness who are steadily building their own fiefdoms treating Nairn like their own latter day colony.
Many Thanks to All the Community Councils in the Highlands that commented against the unwanted merger of NRCC & NW&SCC. It is good that CCs support each other in the face of THC beligerence or when poor planning or inferior developments threaten the well-being of a Community
Update from THC on the results of the the review on CC merger
“Not all questions were mandatory, did not require actual place of residency to be recorded and not every question was fully answered on all the submissions”.
“The total number of responses to the phase 1 Public consultation of the Community Council Scheme of Establishment across Highland was – 96, it is not possible to determine how many were residents from Nairnshire”.
“The total number of responses that indicated they wished to comment on the proposed boundary changes, Highland wide, was 75 and of those 38 indicated that they wished to comment on a change relating to a Nairnshire Community Council”.
“For the proposed merger of Nairn River and Nairn West & Suburban there were 35 responses that indicated that they wished to comment on the proposal, however, only 22 completed the comments question and of those 20 were against the proposal and 2 for the proposal”. – It is clear from this paragraph that the vast majority of those commenting on the Nairn CCs merger were against – a 10-1 ratio is a brilliant result for those who support two independent CCs in Nairn
“Given that the clear majority of those that did respond to the Boundary proposal were against it, it was agreed through the Report to Council not to proceed with the proposal in the 2nd phase of public consultation”.